Who qualifies for
bariatric surgery?
Obesity is a complex health issue. For some people, the most effective solution is bariatric surgery.
You may be a candidate for bariatric surgery if you have:1
There are risks associated with bariatric surgery as with any major procedure. In bariatric procedures, potential risks after surgery may include infection, bleeding, respiratory issues, gastrointestinal leaks, blood clots, and, in rare cases, death.2
Review the potential risks and benefits with your doctor to determine if bariatric surgery is right for you.
Types of Bariatric Surgery
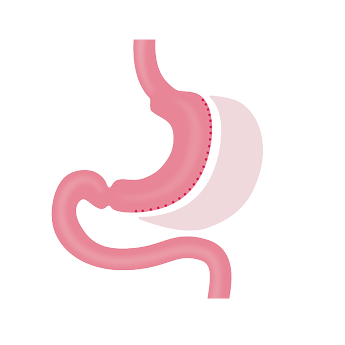
Gastric sleeve is a procedure where the surgeon reduces the stomach by about 80%, leaving a “sleeve” of stomach. No other changes are made to the intestines or digestive system.
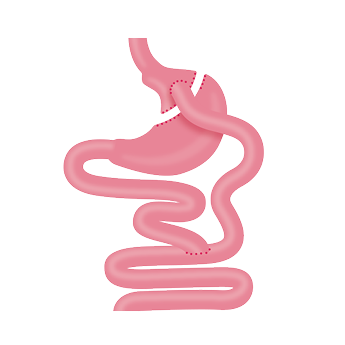
Gastric bypass, also known as Roux-en-Y (roo-en-wy), is a procedure where the surgeon reduces the stomach to a small pouch which is then connected directly to the small intestine.
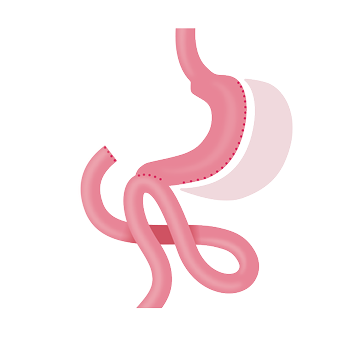
SADI-S, also known as a single anastomosis duodeno-ileal bypass with sleeve gastrectomy, is a procedure where the surgeon performs a sleeve gastrectomy as well as makes one change to the intestines. This surgery reduces the stomach size and impacts the body’s ability to absorb nutrients and calories.
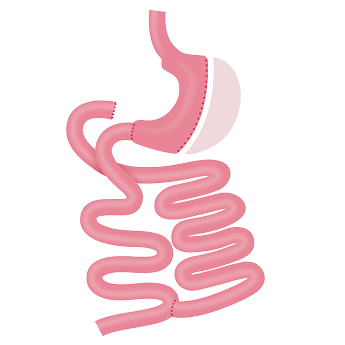
BPD/DS, also known as biliopancreatic diversion with duodenal switch, is a procedure where the surgeon performs a sleeve gastrectomy as well as makes two changes to the intestines. This surgery reduces the stomach size and highly impacts the body’s ability to absorb nutrients and calories.
Malabsorptive bariatric procedures work by limiting the body’s ability to absorb calories, proteins, and nutrients, while restrictive procedures focus on reducing the amount of food consumed and enhancing the sense of fullness after eating.1
The basics about gastric sleeve.
In most bariatric procedures, the size of the stomach is often significantly reduced or a sleeve pouch anatomy is created.
In a sleeve gastrectomy procedure, surgical staplers are used to remove 80% of the stomach, making it much smaller. This reduces the amount of food and liquid the stomach can hold, which helps decrease the amount of calories consumed.1

Potential benefits of the Titan SGS™ Stapler in sleeve gastrectomy.*
*Retrospective data may not be indicative of clinical performance. Individual results may vary.
The Titan SGS™ Stapler is designed to create a consistent, symmetrical sleeve gastrectomy in a single, continuous staple line with only one deployment.4 The approach may contribute to a reduced chance of post-operative complications and shorter hospital stay compared to multi-fire staplers.5,8-11
As the only commercially available U.S. stapler specifically designed for gastric sleeve pouch creation,4,6 the Titan SGS™ Stapler has been used in more than 20,000 procedures.7
Less nausea.8 At 30 days after surgery, 9.2% (72 patients) who had laparoscopic sleeve gastrectomy with the Titan SGS™ Stapler experienced nausea or vomiting, compared to 10.6% (83 patients) with multi-fire staplers (p=0.36).8*
Improved GERD resolution.9 25% of Titan SGS™ Stapler patients who had GERD prior to surgery no longer had GERD 1 year post-op, compared to 10.9% who had a sleeve gastrectomy using multi-fire staplers (p=0.005).9*
† Based on an indirect comparison of operative technique for gastric stapling in the cited published literature for sleeve gastrectomies performed utilizing Covidien and Ethicon Endo-Surgery staplers.

Find a provider
Talk with your doctor about bariatric surgery and if sleeve gastrectomy with the Titan SGS™ Stapler might be right for you.

*Drs. Schram, Foote, authors of the Fritz et al. study and Drs. Morton and Ringold, authors of Ying et al. study, are paid consultants of Teleflex.
Rx only.
The information included on this website is for educational and informational purposes only and should not be used as a substitute for talking to your doctor. Patients should always consult with their doctor about diagnosis or treatment information.
Refer to package insert provided with the product for complete warnings, indications, contraindications, precautions, potential complications and instructions for use.
Teleflex, the Teleflex logo, Standard Bariatrics, and Titan SGS are trademarks or registered trademarks of Teleflex Incorporated or its affiliates, in the U.S. and/or other countries. All other trademarks are the property of their respective owners and are solely used for identification purposes and do not imply any affiliation, endorsement, or ownership by Teleflex Incorporated or its affiliates.